|
| | Deferasirox Chemical Properties |
| Melting point | 260-2620C | | Boiling point | 672.1±65.0 °C(Predicted) | | density | 1.40±0.1 g/cm3(Predicted) | | storage temp. | Keep in dark place,Inert atmosphere,2-8°C | | solubility | Soluble in DMSO (10 mg/ml) | | form | solid | | pka | pKa1 4.57, pKa2 8.71, pKa3 10.56 (Nick); Also reported in H2O/DMSO (CDMSO = 0.20) as pKa1 4.61, pKa2 10.12, pKa3 12.08 (Steinhauser) | | color | Off-white to white | | Stability: | Stable for 2 years from date of purchase as supplied. Solutions in DMSO may be stored at -20°C for up to 1 month. |
| | Deferasirox Usage And Synthesis |
| Overview | Deferasirox: chemical name 4-[3,5-bis (2-hydroxyphenyl)-1,2,4-triazol-1-yl] benzoic acid, is a kind of iron chelator products studied and developed by the Novartis company (Swiss). It was the first routinely used oral iron agent approved by US FDA, allowed to be applied for the treatment of iron overloading caused by blood transfusion in patients (older than 2 years old) of chronic anemia. In Europe, it is recommended as the first-line treatment drug for patients older than 6-year-old who are suffering blood iron overload patients. In China, it is currently subject to clinical research; Ⅱ, Ⅲ clinical trials and pharmacokinetic studies have all shown that it has excellent safety and tolerability, and can significantly reduce the heart, liver iron load, easy to be accepted by the patient. At the same time, it also has pharmacological properties of antifungal (such as Mucor which can grow in iron-ricking environment), anti-cell proliferation, anti-malaria, antioxidant stress injury and anti-cytotoxicity induced apoptosis; it can be used for the treatment of hemochromatosis, delayed skin porphyria and other diseases. | | Preparation | Take salicylic acid as raw material; it undergoes chlorination through thionyl chloride to obtain salicylic acid chloride. Salicylic acid chloride and salicylic acid amide are placed under the condition of high temperature and vacuum distillation instead of ordinary reflux method to obtain intermediates, further evaporating into large amount of low-boiling and by-products through high temperature vacuum distillation, making the mass fraction of the intermediate be increased from 88.7% to 97.5%. Finally, after the removal of hydrochloric acid, the carboxyl-phenylhydrazine hydrochloride is subject to cyclization with the intermediate to prepare the product of deferasirox, reducing the steps of desalting and solvents steaming-off in the post-reaction treatment while reducing the amount of anhydrous ethanol as well so that the operation becomes simpler.
1. Preparation of salicylic acid chloride (Compound 1)
Salicylic acid (13.8 g, 0.1 mol), 10 drops of anhydrous pyridine and 10 mL of thionyl chloride were added to the reaction flask. The mixture was subject to stirred reaction at room temperature for 30 min and slowly heated to 70 °C with stirring until almost no hydrogen chloride gas was released. Further heat to 80 °C and stir for 3 h. Residual thionyl chloride was distilled off under reduced pressure to give a pale yellow liquid which was cooled to precipitate crystals and used directly in the next reaction.
2. Preparation of the 2-(2-hydroxyphenyl)-[1, 3] benzoxazinone (Compound 2)
Salicylic acid (13.7 g, 0.1 mol) and the compound 1 obtained from the last step of reaction are added to the reaction flask equipped with a distillation apparatus and heated to 180 ° C. The reaction mixture was reacted with distillation under reduced pressure at the same time for 3 h to remove water from the reaction. 50 mL of absolute ethanol was added under melting to precipitate the solid yellow product. After filtration and recrystallization from anhydrous ethanol, we can obtain 16.8 g of a yellow product with a yield 70.3% and mp 210-213 °C.
3. Preparation of p-carboxyphenylhydrazine hydrochloride (Compound 3)
4-aminobenzoic acid (6.85 g, 0.05 mol) and 10 mL of distilled water were added into a 250 mL three-necked flask. The mixture was stirred to become a paste and added of drop wise of 12.5 mL of concentrated hydrochloric acid at 5 ° C. The solution was cooled to 5 ° C in an ice-salt bath. Upon stirring, slowly add drop wise of a sodium nitrite saturated solution (3.5 g, 0.05 mol of sodium nitrite is dissolved in a small amount of water (8 g)) for diazotization reaction. The reaction temperature is kept below 5 ℃ and further stirred for 30 mins after the completion of dropping.
The diazonium salt solution was then poured into a solution with sodium sulfite (25.2 g, 0.2 mol) dissolved in water (100 mL) pre-cooled to 5 °C. Stir at this temperature for 30 min, and heat to 80 ° C for 1.5 h. The orange-red solution will be changed to yellowish. Cool it to room temperature; slowly add hydrochloric acid for acidification to pH 3 to obtain the p-carboxyphenylhydrazine hydrochloride precipitate. Further apply filtration and drying to get 8.3 g white product with a yield of 88.3%.
4. Preparation of Deferasirox
The compound 3 (3.8 g, 0.02 mol) was adjusted to pH 6 with 30% NaOH, stirred, and stand for layering so that the water layers were separated. The oil layer was p-carboxyphenylhydrazine. The oil layer was placed in a flask; add compound II (5.0 g; 0.02 mol) and reflux for 2 h in anhydrous ethanol (75 mL). Cool, precipitate the crystals; filtrate and rinse with 10 mL of ice ethanol, dry and perform ethanol-water recrystallization, to obtain 6.3 g micro-yellow product with a yield of 84.45%.

Figure 1 synthetic route of Deferasirox | | Pharmacological effects | DFS has antifungal activity (such as Mucor growing in the iron-rich environment), anti-cell proliferation, anti-malaria, anti-oxidative stress injury, anti-cytotoxicity induced apoptosis and other pharmacological effects.
1. DFS and fungal infection
Iron is a substance that fungi rely on, and plays a very important role in the growth and toxicity of fungi. The antifungal effect of iron chelator may be due to their effect of removal of the iron necessary for fungal growth, so as to achieve the purpose of treatment of fungal infection.
2. DFS and cell proliferation
Iron plays a very important role in the process of cell proliferation. Iron chelators may have anti-proliferative properties, suggesting that iron chelators may be a novel anticancer agent for the treatment of tumors. | | Pharmacokinetics | DFS is a tridentate iron chelator that binds ferric ions in a 2: 1 ratio to form complexes that are excreted from the feces, reducing the storage of iron in the body. As DFS persists in plasma, the plasma non-transferring binding iron can be continuously reduced, thus directly eliminating the iron toxicity formed in vivo. The main metabolic pathway of DFS is via glucuronidation for producing metabolites M3 (acylglucuronide) and M6 (2-O-glucuronide).
Administration of large-dose DFS may present some acute adverse reactions, such as gastrointestinal symptoms (15%) and rash (11%). However, patients who finally discontinue the drug treatment due to these symptoms are rare. | | Side effects | For patients with renal insufficiency, DFS can lead to increased creatinine levels with 38% of patients getting creatinine levels increased by 33% or more. But DFS-induced creatinine increase will generally not exceed the normal upper limit and there has not yet been progress in renal disease reported. After a reduction in DFS, creatinine levels returned to normal or remained stable in 13% of patients.
<1% of patients can get hearing impairment (hearing loss, hearing reduction) and ocular diseases (lens opacities, cataracts, elevated intraocular pressure and retinopathy), and therefore it is recommended to participate into hearing and visual capability examination (including slit lamp examination and fundus examination)annually before and during the period of iron therapy, once found, it should be considered to disable DFS.
Common side effects of deferasirox in Chinese patients with thalassemia include: rash, abdominal pain, diarrhea, and elevated transaminase level and serum creatinine level; mostly mild with no serious adverse reactions.
Deferasirox can cause renal damage and gastrointestinal bleeding, and therefore it is recommended to detect 2 times of creatine clearance rates before the treatment; detect once per week during the initial stage of treatment, followed by once per month. Gastrointestinal bleeding is a common adverse reaction of this drug that can be fatal in older patients with advanced malignancies or thrombocytopenia, and these patients are unlikely to benefit from the treatment with this drug.
Deferasirox may lead to serious adverse effects of liver failure. The patient must subject to regular monitoring of liver function during the medication process. If there is difficult to explain, persistent or progressive increase on the serum aminotransferase levels, we should adjust the usage or withdraw the drug. | | Uses | 1. DFS can be used to treat the reversible renal insufficiency caused by Fanconi syndrome.
2. It can be used for the treatment of secondary hemochromatosis.
3. It can be used for the treatment of delayed skin porphyria.
4. It can be used for the treatment of myelodysplastic syndromes.
5. It can be used for the treatment of iron overloading caused by blood transfusion for patients (older than 2 years old) of chronic anemia This information is compiled and edited by Ding Hong of Chemicalbook. (2015-09-18) | | Precautions | Patients with allergy to deferasirox are disabled. | | Description | Linagliptin was originally discovered at Boehringer Ingelheim as
an orally active dipeptidyl peptidase-IV (DPP-4) inhibitor. Eli Lilly
and Boehringer Ingelheim co-developed and launched linagliptin
for type II diabetes as an adjunct to diet and exercise for the
improvement of adult glycemic control. Linagliptin has a superior
DPP-4 IC50 value of 1 nM, compared with 19 nM for sitagliptin,
24 nM for alogliptin, 50 nM for saxagliptin and 62 nM for vildagliptin. In addition, linagliptin exhibited prolonged pharmacodynamic
activity with long-lasting DPP-4 inhibition in several
preclinical species. Linagliptin showed good efficacy in phase II
clinical trials with doses as low as 5 mg and no signs of hypoglycemia
with doses as high as 600 mg. The prolonged pharmacological
effect of DPP-4 activity and the good safety/tolerability profile
provided the basis for linagliptin’s approval. | | Chemical Properties | White to Off-White Solid | | Originator | Novartis (Switzerland) | | Uses | A tridentate chelator that binds iron with high affinity | | Uses | Orally active tridentate iron chelator | | Uses | Labeled Deferasirox, intended for use as an internal standard for the quantification of Deferasirox by GC- or LC-mass spectrometry. | | Uses | Biological Activity Chemical Information Tech Support & FAQs
Biological Activity
Deferasirox(Exjade) is a rationally-designed oral iron chelator. Its main use is to reduce chronic iron overload in patients who are receiving long-term blood transfusions | | Definition | ChEBI: A member of the class of triazoles, deferasirox is 1,2,4-triazole substituted by a 4-carboxyphenyl group at position 1 and by 2-hydroxyphenyl groups at positions 3 and 5. An orally active iron chelator, it is used to manage chronic iron overload in patient
receiving long-term blood transfusions. | | Brand name | Exjade (Novartis). | | Clinical Use | Treatment of iron overload | | Synthesis | Synthesis of deferasirox started with cyclization of salicylamide (26) with salicyloyl
chloride (27) by heating at 170 C without any solvents to
give 2-(2-hydroxyphenyl)-benz[e]oxazin-4-one (28) in
55% yield. Compound 28 was reacted with 4-hydrazinobenzoic
acid (29) in refluxing ethanol for 2 hours to give
deferasirox V as colorless crystals. 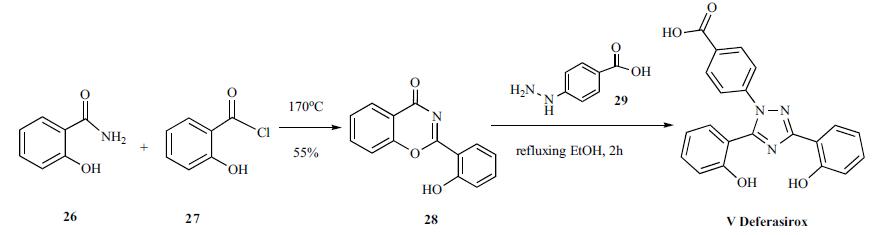
| | Drug interactions | Potentially hazardous interactions with other drugs
Aluminium-containing antacids: avoid concomitant
use.
Aminophylline and theophylline: concentration of
aminophylline and theophylline increased, consider
reducing aminophylline and theophylline dose.
Other nephrotoxic agents: avoid concomitant
therapy | | Metabolism | Metabolism of deferasirox is mainly glucuronidation by
uridine diphosphate glucuronosyltransferase (UGT)
enzymes. Cytochrome P450 isoenzyme-mediated
metabolism appears to be minor. Deconjugation of
the glucuronidates in the intestine and subsequent
enterohepatic recycling are likely to occur.
It is excreted mainly in the faeces via bile, as metabolites
and as unchanged drug. About 8% of a dose is excreted in
the urine. | | References | Heinz et al. (1999), 4-[3,5-Bis(2-hydroxyphenyl)-1,2,4-triazol-1-yl]-benzoic acid: A Novel Efficient and Selective Iron(III) Complexing Agent; Ang. Chem. Int. Ed., 38 2568
Palumbo et al. (2021), From Biology to Clinical Practice: Iron Chelation Therapy With Deferasirox; Front. Oncol., 11 752192
Roatsch et al. (2019), The Clinically Used Iron Chelator Deferasirox Is an Inhibitor of Epigenetic JumonjiC Domain-Containing Histone Demethylases; ACS Chem. Biol., 14 1737
Lui et al. (2015), Targeting cancer by binding iron: Dissecting cellular signaling pathways; Oncotarget, 6 18748
Ibrahim and O’Sullivan (2020), Iron chelators in cancer therapy; Biometals, 33 201
Szymonik et al. (2021), The Impact of Iron Chelators on the Biology of Cancer Stem Cells; Int. J. Mol. Sci., 23 89 |
| | Deferasirox Preparation Products And Raw materials |
|


