|
| | Etoricoxib Chemical Properties |
| Melting point | 134-135°C | | Boiling point | 510.0±50.0 °C(Predicted) | | density | 1.298±0.06 g/cm3(Predicted) | | storage temp. | Inert atmosphere,2-8°C | | solubility | DMSO : 100 mg/mL (278.68 mM; Need ultrasonic) | | pka | 4.5(at 25℃) | | form | neat | | BRN | 8073797 | | InChIKey | MNJVRJDLRVPLFE-UHFFFAOYSA-N | | CAS DataBase Reference | 202409-33-4(CAS DataBase Reference) |
| Hazard Codes | T | | Risk Statements | 22-24 | | Safety Statements | 36/37-45 | | RIDADR | UN 2811 6.1 / PGII | | WGK Germany | 3 |
| | Etoricoxib Usage And Synthesis |
| Cyclooxygenase -2 (COX-2) inhibitors | Etoricoxib is a kind of highly selective cyclooxygenase-2 (COX-2) inhibitors developed by the Merck company with the chemical name being 5-chloro-6'-methyl-3-4-(methanesulfonamide) phenyl]-2, 3'-bipyridine. Etoricoxib has a unique chemical structure that is methylsulfonyl group. The introduction of this group can not only increase the selectivity for COX-2 drugs, but also does not produce sulfa drugs and cross-allergic reactions. Etoricoxib was first approved for entering into market in 2002 in the UK, followed by the marketing countries and regions including the European Union, Asia, Australia and Latin America. Until the end of 2013, it has been approved for marketing in 97 countries for being widely used in treatment of osteoarthritis (OA), rheumatoid arthritis, ankylosing spondylitis, chronic low back pain, acute gouty arthritis, primary dysmenorrhea and postoperative pain, and other diseases. Etoricoxib has also entered into market in Taiwan and Hong Kong of China. It had entered into market in Chinese mainland in 2008 with the approved indications being acute gouty arthritis and OA and another indication being primary dysmenorrhea in the second half year of 2014.
| | Pharmacological effects | Etoricoxib is a non-steroidal anti-inflammatory drug with anti-inflammatory, analgesic and antipyretic effects in animal models. It is a kind of orally active, selective cyclooxygenase-2 inhibitor within the clinical dose range or higher doses. It has already confirmed of two subtypes of cyclooxygenase: cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2). COX-1 is involved in the prostaglandin mediated normal physiologic functions such as gastric cytoprotection and platelet aggregation. Non-selective non-steroidal anti-inflammatory drugs inhibit the generation of COX-1, and thus can cause gastric mucosal injury and decreased platelet aggregation. COX-2 is mainly involved in the production of prostaglandins, and prostaglandins can cause pain, inflammation and fever. Etoricoxib is a kind of selective COX-2 inhibitors which can reduce these symptoms and signs as well as reduce gastrointestinal side effects without affecting platelet function.
The above information is edited by the chemicalbook of Dai Xiongfeng.
| | Pharmacokinetics | Absorption: it has excellent oral absorption with the mean oral bioavailability being close to 100%. For adult, it can be subject to oral administration of 120mg upon empty stomach for once daily until it reaches steady state. Its plasma concentration reaches peak in about 1 hour after drug administration. This pharmacokinetic of this product exhibits linear correlation within clinical dose range.
Distribution: in the concentration range 0.05-5mcg/ml; 92% binds to human plasma protein. In the human body, volume of distribution at steady state is approximately 120 liters. It can penetrate the placenta of rats and rabbits as well as the blood-brain barrier in rats.
Metabolism: Metabolic is complete with the proto-drug content in the urine being less than 1%. The main metabolic pathway is through the catalysis through the enzyme cytochrome P450 (CYP), forming a six-carboxylic acid derivative.
Clearance: In healthy individuals, intravenous administration of radio-labeled Etoricoxib; 70% of the radioactivity could be detected in the urine, 20% of the radioactivity could be detected in the feces while most of them being in the form of the presence of metabolites and only less than 2% of the prototype drug is excreted.
| | Drug Interactions | Warfarin: long-term usage of warfarin therapy in patients with stable efficacy. Daily application of this drug should be 120mg with the prothrombin time being approximately 13% higher than the international normalized ratio (INR).
Rifampicin: Rifampicin is a strong inducer of hepatic metabolism. The combination of this product with rifampicin allows the plasma area under the curve (AUC) to be reduced by 65%. Therefore when this product is combined with rifampin, we should take into account their interaction.
Methotrexate: When using this product at a dose greater than 90mg/day as well as being in combination with methotrexate, you should consider monitoring the toxicity associated with methotrexate.
Diuretics, angiotensin-converting enzyme (ACE) inhibitors and angiotensin II antagonists (AIIAs): Non-steroidal anti-inflammatory drugs, including selective cyclooxygenase-2 inhibitors can reduce the antihypertensive effect of the diuretics, angiotensin converting inhibitors and angiotensin II antagonists.
Lithium salt: non-selective non-steroidal anti-inflammatory drugs and cyclooxygenase-2 selective inhibitors may increase plasma levels of lithium salts.
Aspirin: It can be used simultaneously with a lose-dose aspirin for the prevention of cardiovascular events. However, upon being in combination with low-dose aspirin, the incidence of gastrointestinal ulcers or other complication rate is higher than in the case of single usage of this product.
Oral contraceptives: upon selecting suitable oral contraceptives for being used in combination with this product, we need to take into account of the increase of the EE concentration. The increase of the EE concentration will increase the incidence of the related adverse events of oral contraceptives (such as the risk of venous thromboembolism for women).
Other: Antacids and ketoconazole (CYP3A4 strong inhibitors) do not produce clinically significant impact on the pharmacokinetics of this product.
| | Indications | 1. the treatment of OA: the good has a comparable effect as celecoxib, ibuprofen with similar efficacy with large doses of diclofenac and naproxen.
2. acute gouty arthritis: This product is 120 mg/d and can quickly and effectively relieve pain, and has a similar efficacy as the gold standard drug indomethacin in the treatment of gouty arthritis with a better tolerance and a lower incidence of drug-related adverse events than indomethacin.
3. ankylosing spondylitis: etoricoxib has a similar efficacy as naproxen taken twice per day; etoricoxib has a better effect in treating secondary end-point aspects such as alleviating night pain, inflammation, functionality and flexibility.
4. rheumatoid arthritis: large-scale, controlled clinical trial results showed that etoricoxib taken once daily has a better efficacy compared to naproxen taken twice daily with a better tolerance in patients.
5. osteoarthritis: This product (once/day) has a comparable efficacy as celecoxib (once/day), and ibuprofen (3 times/day); and it (once/day) has a similar efficacy with high-dose diclofenac (3 times/day) and naproxen (3 times/day).
6. postoperative dental pain: compared with acetaminophen/codeine and oxycodone/ p-acetaminophen, taking etoricoxib once daily can yield a better efficacy in alleviating the pain feeling of patients.
7. chronic low back pain: compare this product with Placebo on the treatment efficacy of chronic low back pain in 12 weeks has demonstrated that the clinical efficacy of this product was significantly superior to placebo drug with being effective in the treatment for only one week while the effect is very significant in four weeks and the sustained effect being able to reach over three months.
8. for controlling late pain of postoperative thyroid: when thyroid operation patients orally take etoricoxib at 1 h before operation can reduce the oral administrated dose of oxycodone acetaminophen at 6~12 h after surgery in patients.
| | Safety | Compared with diclofenac, the incidence of this product in inducting thrombotic cardiovascular events has no significant difference while the cumulative incidence of clinically diagnosed gastrointestinal perforation, ulcers, bleeding in etoricoxib group was significantly lower than the diclofenac group. The incidence of gastrointestinal adverse events is decreased by 50% compared with the diclofenac sodium. Etoricoxib has a low gastrointestinal reaction. During the treatment, the gastrointestinal symptoms (nausea, vomiting, abdominal pain or discomfort, diarrhea), chest and ankle edema and other adverse events for etoricoxib is similar to other selective COX-2 inhibitors. It is contraindicated in patients with ischemic heart disease and stroke. For patients with risk factors such as heart disease, they should use with caution.
| | Description | Etoricoxib is a COX-2 inhibitor developed as a follow-up of rofecoxib for the treatment
of osteoarthritis, rheumatoid arthritis, dysmenorrhoea, gout, ankylosing spondylitis and
pain. Several processes describe the preparation of etoricoxib in 4 or 5 steps from 6-
methylnicotinate. The key step is the novel pyridine construction using annulation of a
ketosutfone with a vinamidinium synthon. In human whole blood, in vitro, the IC50 value
obtained for inhibition of COX-2 is 1 .I μM as compared to 116 μM obtained for inhibition of
COX-1. Thus, etoricoxib is the most selective COX-2 inhibitor to date, with a COX-IKOX-
2 ratio of IC50 values of 106 for etoricoxib as compared to 35, 30, 7.6 for rofecoxib,
valdecoxib and celecoxib, respectively. Its in vivo potency is generally comparable to that
of rofecoxib in animal models against inflammation (carrageenan-induced paw edema),
pyrexia (LPS-induced pyresis), pain (carrageenan-induced hyperalgesia) and arthritis
(adjuvant-induced arthritis). Etoricoxib is well tolerated with dose-proportional
pharmacokinetics. It has no effect on bleeding time or platelet ag regation. The
gastrointestinal tolerability of etoricoxib is excellent as demonstrated by [51Cr] models of
excretion in rats and squirrel monkeys. Moreover, etoricoxib, unlike naproxen is not
associated with significant inhibition of gastric mucosal PGE2 synthesis compared to
placebo. Etoricoxib is highly absorbed, has a tmax of 1.5 h and a half-life time of
approximately 15-22h. Five metabolites, weak inhibitors of COX-1 and COX-2 have been
identified after renal excretion. Finally, although multiple CYP enzymes are involved in the
metabolism of etoricoxib (CYP3A4 being the major contributor), etoricoxib is not a potent
CYP3A4 inhibitor or inducer. In patients undergoing molar extraction, etoricoxib showed
similar efficacy to naproxen sodium with a longer duration of analgesia than
acetaminophen/codeine (approximately >24 h, 22 h and 5.2 h, respectively) and a better
total pain relief score over 8 h. Similar efficacy of etoricoxib and naproxen was also seen in
patients suffering of osteoarthritis. In the treatment of rheumatoid arthritis and ankylosing
spondylitis, etoricoxib demonstrated significantly superior efficacy compared to naproxen
and placebo. Etoricoxib did not affect the pharmacokinetics of prednisolone (i.v. or p.0.)
and its co-administration with antacids showed insignificant effects on the maximal
concentration and its absorption.
. | | Chemical Properties | Off-White Powder | | Originator | Merck & Co (USA) | | Uses | For the treatment of rheumatoid arthritis, osteoarthritis, ankylosing spondylitis, chronic low back pain, acute pain and gout. | | Uses | anti-inflammatory, analgesic;cyclooxygenase inhibitor | | Uses | Etoricoxib is a dipyridinyl compound that demonstrates high in vitro and ex vivo selectivity for COX-2 over COX-1 in several assays, e.g., in the production of PGE2 by CHO cells expressing either COX-2 (IC50 = 79 nM) or COX-1 (IC50 > 50 μM). Oral etoricoxib is well absorbed and metabolized extensively via oxidation, with metabolites excreted largely in the urine.[Cayman Chemical] | | Uses | A specific inhibitor of COX-2 .
| | Uses | Labeled Etoricoxib, intended for use as an internal standard for the quantification of Etoricoxib by GC- or LC-mass spectrometry. | | Definition | ChEBI: A member of the class of bipyridines that is 2,3'-bipyridine which is substituted at the 3, 5, and 6' positions by 4-(methylsulfonyl)phenyl, chlorine, and methyl groups, respectively. | | Brand name | Arcoxia | | Pharmacokinetics | Etoricoxib is rapidly
absorbed, with an oral bioavailability of 80 to 100%, and reaches maximum plasma concentrations in 1 to 2 hours
after dosing. Food decreases the rate of absorption but has no effect on the extent of absorption. It exhibits a long
elimination half-life of approximately 22 hours, demonstrating linear plasma pharmacokinetics with no accumulation
during multiple dosing. | | Clinical Use | Etoricoxib is a selective COX-2 inhibitor being developed for postsurgical treatment of dental pain (120
mg) and osteoarthritis. It has a methylsulfonyl group common to the other coxib inhibitors. | | Synthesis | The synthesis of etoricoxib (8) was explored extensively by
the Merck process research group. Key intermediate 85
was synthesized through at least three different routes. In the
Horner-Wittig approach, 6-methyl methylnicotinate (79) was
converted into Weinreb amide 80 in 95% yield. Amide 80
was then converted to aldehyde 81 via a DIBAL-H mediated
reduction. Subsequent treatment of a solution of aldehyde 81
in isopropyl acetate with aniline and diphenyl phosphite
provided N,P-acetal 82 in 87% yield. The Horner-Wittig
reaction of N,P-acetal 82 with 4-methanesulfonylbenzaldehyde
(83) furnished enamine 84, which was
hydrolyzed to ketosulfone 85. A Grignard approach was also
developed in the preparation of ketosulfone 85. Addition of
Grignard reagent 86 to Weinreb amide 80 in toluene/THF
provided ketosulfide 85 in 80% yield. Tungstate-catalyzed
oxidation of ketosulfide 87 using hydrogen peroxide
provided ketosulfone 85 in 89% yield by simple filtration.
Ketosulfone 85 was prepared through Claisen condensation
protocol as well. Thus, reaction of 4-methanesulfonyl phenyl
acetic acid (88) with methyl nicotinate 79 under Ivanoff
condition, i.e., the magnesium dianion in THF, resulted
58% yield of ketosulfone 85. Treatment of ketosulfone 85
with a three-carbon electrophile, 2-chloro-N,Ndimethylaminotrimethinium
hexafluorophos-phate (89) in
the presence of potassium t-butoxide at ambient temperature
resulted adduct 90. Inverse quench of adduct 90 into a
mixture of HOAc /TFA led to the putative intermediate 91.
Ring closure of the pyridine ring occurred upon heating at reflux in the presence of an excess of aqueous ammonium
hydroxide to give desired etoricoxib (8) in 97% yield in a
one-pot process from 85. 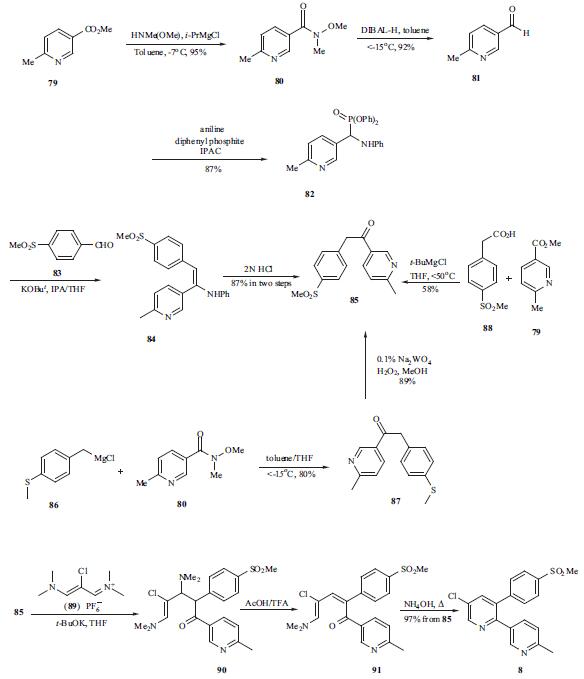
| | Drug interactions | Potentially hazardous interactions with other drugs
ACE inhibitors and angiotensin-II antagonists:
antagonism of hypotensive effect; increased risk of
nephrotoxicity and hyperkalaemia.
Analgesics: avoid concomitant use of 2 or more
NSAIDs, including aspirin (increased side effects);
avoid with ketorolac, increased risk of side effects and
haemorrhage.
Antibacterials: possibly increased risk of convulsions
with quinolones; concentration reduced by
rifampicin.
Anticoagulants: effects of coumarins and
phenindione enhanced; possibly increased risk of
bleeding with heparin, dabigatran and edoxaban -
avoid long term use with edoxaban.
Antidepressants: increased risk of bleeding with
SSRIs and venlaflaxine.
Antidiabetic agents: effects of sulphonylureas
enhanced.
Antiepileptics: possibly increased phenytoin
concentration.
Antivirals: increased risk of haematological toxicity
with zidovudine; concentration possibly increased by
ritonavir.
Ciclosporin: may potentiate nephrotoxicity
Cytotoxics: reduced excretion of methotrexate;
possibly reduced excretion of pemetrexed; increased
risk of bleeding with erlotinib.
Diuretics: increased risk of nephrotoxicity;
antagonism of diuretic effect; hyperkalaemia with
potassium-sparing diuretics.
Lithium: excretion decreased.
Pentoxifylline: increased risk of bleeding.
Tacrolimus: increased risk of nephrotoxicity. | | Metabolism | Etoricoxib is metabolized involving oxidation of its 6′-methyl group primarily by CYP3A4 but is
not an inhibitor of CYP3A4. Other metabolites include 1′-N-oxide and glucuronides. Etoricoxib is primarily excreted as
metabolites into the urine. |
| | Etoricoxib Preparation Products And Raw materials |
|


